2020 Expert Consensus Decision Pathway on Novel Therapies for Cardiovascular Risk Reduction in Patients With Type 2 Diabetes J Am Coll Cardiol 2020;76:1117–45
將基礎胰島素(Human NPH 或一種長效胰島素類似物)添加到口服藥物治療,是有效的方式。最近的證據支持 GLP-1 RA 在未達到血糖目標的患者中的效用。
大多數 GLP-1 RA 是可注射的,但Semaglutide的口服製劑現已上市。在比較需要進一步降低血糖的患者中添加注射用 GLP-1 RA 或胰島素的研究中,注射用 GLP-1 RA 的血糖功效與基礎胰島素相似或更高。在這些研究中,與胰島素相比,GLP-1 RA 的低血糖風險和對體重的有益影響較低,但胃腸道副作用更大。因此,研究結果支持 GLP-1 RA 是需要注射療法以控制血糖的患者的首選治療方式(Fig 9-4)。
在強化胰島素治療的患者中,與單獨使用胰島素強化治療相比,GLP-1 RA 併用治療已被證明具有更高的血糖治療效果和持久性。然而,成本和耐受性問題是 GLP-1 RA 使用中的重要考慮因素。
Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet 2019 Oct 26;394(10208):1519-1529.
Pratley R, Amod A, Hoff ST, et al.; PIONEER 4 investigators. Oral semaglutide versus subcutaneous liraglutide and placebo in type 2 diabetes (PIONEER 4): a randomised, double-blind, phase 3a trial. Lancet 2019;394:39–50
Gerstein HC, Sattar N, Rosenstock J, et al.; AMPLITUDE-O Trial Investigators. Cardiovascular and renal outcomes with efpeglenatide in type 2 diabetes. N Engl J Med 2021;385:896–907
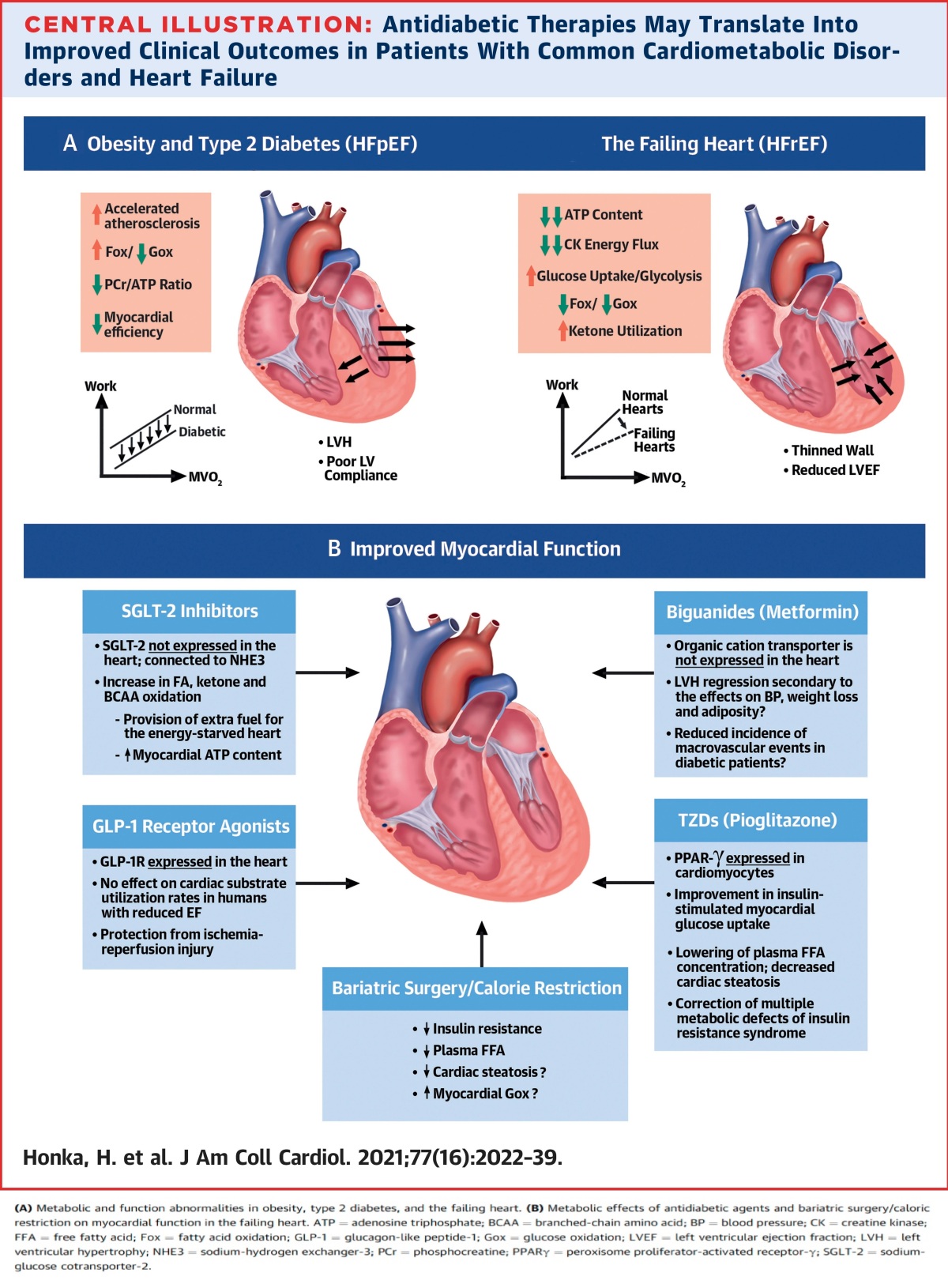
心肌葡萄糖的吸收是由跨質膜的葡萄糖梯度(Gradient)和質膜中葡萄糖轉運蛋白驅動。胰島素,運動和局部缺血會刺激該過程,FAs會抑制這一過程。一旦進入心肌細胞,葡萄糖就會進行糖分解,從而產生2個丙酮酸(pyruvate),2個ATP和2個NADH分子。糖分解的限速酶是磷酸果糖激酶-1 (phosphofructokinase-1),可被ATP,檸檬酸和降低的組織pH抑制。相反,通過運動和局部缺血激活AMPK (adenosine monophosphate-activated protein kinase) 可以通過激活phosphofructokinase-2,產生果糖2,6-雙磷酸酯 (fructose2,6-bisphosphate) 來刺激糖分解通量。
丙酮酸脫羧酶由限速酶丙酮酸脫氫酶(PDH, pyruvate dehydrogenase)催化,通過PDH的通量與心肌葡萄糖攝取的速率相對應。PDH的主調節器通量,因此,在正常條件下葡萄糖氧化是脂肪酸氧化。PDH被PDH激酶(PDK)去除活性,PDK激酶受細胞能量狀態的控制。NADH / NAD +acetyl-CoA/free CoA 的比例增加會刺激PDK,導致通過PDH的通量減少,丙酮酸氧化減少。降低NAD +檸檬酸介導的PFK-1抑制是FAs和酮類與碳水化合物氧化競爭的重要生化機制。在充分灌注的條件下,丙酮酸轉化為乳酸的重要性很小。
在NYHA Fc III的心衰竭病人,於冠狀動脈內輸注丙酮酸(pyruvate),可以改善38%之心搏出量,及降低36%之肺楔壓。此外,NYHA Fc III-IV的心衰竭病人中,輸注30分鐘的二氯乙酸鹽(dichloroacetate)(一種PDH激酶的特異性抑製劑)可增加心肌乳酸的攝取和心搏出量,並將心肌耗氧量從19.3 ml /min降低至16.5 ml /min。這些數據表明,提供能量匱乏之衰竭中的心臟,使用代謝效率更高的燃料可以改善心肌ATP含量和LV收縮功能。值得注意的是,通過刺激丙酮酸的氧化(pyruvate oxidation) 而增加的心臟功能與使用傳統的血管增壓劑所觀察到的相似,但是沒有任何負能量消耗。
GLP-1 RA : glucagon-like peptide-1 receptor agonist 升糖素樣肽1受體增強劑
MACE: major adverse cardiovascular event
MVO 2 : myocardial oxygen consumption心肌耗氧量
P/O ratio: phosphorus/oxygen ratio磷/氧比
資料來源:
J Am Coll Cardiol 2021, 77(16) 2022-2039
References:
Kristensen SL, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol 2019;7:776–85.
Lincoff AM, Wolski K, Nicholls SJ, Nissen SE. Pioglitazone and risk of cardiovascular events in patients with type 2 diabetes mellitus: a meta analysis of randomized trials. JAMA 2007;298:1180–8.
Dormandy JA, et al.Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive study (PROspective pioglitAzone clinical trial in macroVascular events): a randomised controlled trial. Lancet 2005;366:1279–89.
Mohan M, et al. A randomized controlled trial of metformin on left ventricular hypertrophy in patients with coronary artery disease without diabetes: the METREMODEL trial. Eur Heart J 2019;40:3409–17.
Strongman H, et al.Pioglitazone and cause-specific risk of mortality in patients with type 2 diabetes: extended analysis from a European multi-database cohort study. BMJ Open Diabetes Res Care 2018;6:e000481
Zinman B, Lachin JM, Inzucchi SE. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2016;374:1094
Neal B, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017; 377:644–57.
Wiviott SD, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019;380:347–57
Marso SP, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016;375:311–22.




















你必須登入才能發表留言。